SOFA vs SIRS and sonographic features of septic shock in dogs
In human medicine concepts in sepsis have evolved.
SIRS:
In 2016, a new consensus termed Sepsis-3 removed the concept of SIRS from the sepsis definition and replaced it with the SOFA (Sequential [Sepsis-Related] Organ Failure Assessment) score.
The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).
JAMA. 2016; 315(8):801-10 (ISSN: 1538-3598)
Singer M; Deutschman CS; Seymour CW; Shankar-Hari M; Annane D; Bauer M; Bellomo R; Bernard GR; Chiche JD; Coopersmith CM; Hotchkiss RS; Levy MM; Marshall JC; Martin GS; Opal SM; Rubenfeld GD; van der Poll T; Vincent JL; Angus DC
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4968574/
This change increased specificity but decreased sensitivity. However, the authors stated that the SIRS criteria should continue to aid in the general diagnosis of infection.
Sepsis:
Prior to 2016 sepsis was defined as suspected/known infectious with two or more SIRS criteria. In 2016, the definition in human medicine was altered to ‘a life-threatening organ dysfunction caused by a dysregulated response to infection.’
Organ dysfunction was defined by an acute change in Sequential (Sepsis-Related) Organ Failure Assessment (SOFA) score.
Severe Sepsis:
Prior to 2016, severe sepsis was defined as SIRS to infection associated with organ dysfunction with manifestations of hypoperfusion and/or hypotension. In 2016, this term was abandoned as it was deemed superfluous based on the new sepsis definition in human medicine.
Septic Shock:
Prior to 2016, SIRS to infection with hypotension refractory to volume resuscitation. In 2016, septic shock in human medicine was re-categorized as a subset of sepsis characterized by persistent hypotension requiring vasopressors to maintain mean arterial pressure (MAP) >65 mmHg.
Multiple Organ Dysfunction Syndrome (MODS):
MODS is defined as altered function of two or more organs secondary to SIRS such that homeostasis can’t be maintained without intervention.
-Ψ-
SOFA scoring for dogs has been discussed in the veterinary literature as far back as 2012:
Schweiz Arch Tierheilkd. 2012 Aug;154(8):325-30
Application of the Sequential Organ Failure Assessment Score to predict outcome in critically ill dogs: preliminary results.
Ripanti D1, Dino G, Piovano G, Farca A.
https://www.ncbi.nlm.nih.gov/pubmed/22851431
Abstract
In human medicine the Sequential Organ Failure Assessment (SOFA) score is one of the most commonly organ dysfunction scoring systems used to assess critically ill patients and to predict the outcome in Intensive Care Units (ICUs). It is composed of scores from six organ systems (respiratory, cardiovascular, hepatic, coagulation, renal, and neurological) graded according to the degree of the dysfunction. The aim of the current study was to describe the applicability of the SOFA score in assessing the outcome of critically ill dogs. A total of 45 dogs admitted to the ICU was enrolled. Among these, 40 dogs completed the study: 50 % survived and left the veterinary clinic. The SOFA score was computed for each dog every 24 hours for the first 3 days of ICU stay, starting on the day of admission. A statistically significant correlation between SOFA score and death or survival was found. Most of the dogs showing an increase of the SOFA score in the first 3 days of hospitalization died, whereas the dogs with a decrease of the score survived. These results suggest that the SOFA score system could be considered a useful indicator of prognosis in ICUs hospitalized dogs.
-Ψ-
I must admit that I find SIRS criteria a bit of a blunt instrument in dogs. Since respiratory rate and heart rate are affected by lots of other variables as well as sepsis, and fever is not terribly specific either, it tends to rely a lot on white blood cell count. Cut-off values for wbc numbers are not backed by hard evidence the low end is usually quoted as around 4-5 x 10^9/l and the top end 16-19 x 10^9/l. SOFA score feels a bit more rigorous……although at the moment I feel that it’s best used more as a broad concept rather than an objective numerical assessment.
Point-of-care ultrasound (POCUS) offers a convenient way to quickly assess some of the important target organ systems in sepsis.
Heart:
This is the heart of a 12 y.o. Weimaraner with extensive, acute, bilateral pneumonia.
The ratio of LV internal diameter:wall thickness at end-diastole should be at least 3.5:1. This dog registers <1:1. There is no evidence of LV outflow tract obstruction and in the circumstances ‘pseudohypertrophy’ due to hypotension is overwhelmingly likely to be the cause of this appearance. Systolic function is markedly subnormal.

Lung ultrasound from the same patient: there are large areas of irregularly-marginated consolidation (‘shred sign’) with air bronchiolograms characteristic of pneumonia.
Although the evidence is circumstantial, I suspect that pneumonia is the primary cause of this patient’s problem. Consolidation suggests pneumonia rather than sepsis-induced lung injury (acute respiratory distress syndrome [ARDS]/ acute lung injury [ALI]) which normally manifests as a diffuse increase in B lines.
Gut:
The gut is not only a potential source of infection in sepsis; it is also an important target organ.
Am J Physiol Gastrointest Liver Physiol. 2004 Sep;287(3):G685-94.
Mechanisms of polymicrobial sepsis-induced ileus.
Overhaus M1, Tögel S, Pezzone MA, Bauer AJ.
https://www.ncbi.nlm.nih.gov/pubmed/15331356
‘
‘the intestine is not only a source of bacteremia but also an important target of bacterial products with major functional consequences to intestinal motility and the generation of cytokines, which participate in the development of multiple organ failure‘.
i.e. ileus.
Thus, in this canine patient with severe pneumonia, the stomach is hypomotile and distended with gas:
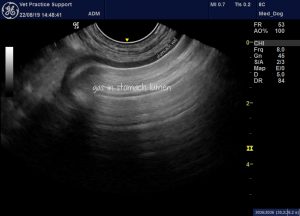
In fact, collapse with apparent abdominal pain was the presenting complaint in this dog.
The colon contains small amounts of liquid diarrhoea and gas bubbles. The wall is diffusely, mildly thickened.

Liver:

We can’t be sure that this liver change is part of a syndrome of MODS rather than some other process. However, diffuse, patchy, hypoechoic change would be consistent with acute hepatopathy.

There is apparent gallbladder wall oedema.



