Persistent left cranial vena cava amongst multiple congenital cardiac defects in a cat
This poor chap was a British Short-Hair and 3 y.o. at presentation. He was presented for progressive weight loss with polyuria/polydispsia and proved to be azotaemic. However, his kidneys are another story -we are concerned here with his heart. On physical examination he proved to have systolic murmurs on both left and right sides about grade III and a gallop sound.
His lung fields appear ultrasonographically free from pulmonary oedema. However, there is evidence of right sided congestive failure in that the caudal vena cava at the level of the diaphragm fails to collapse on inspiration:
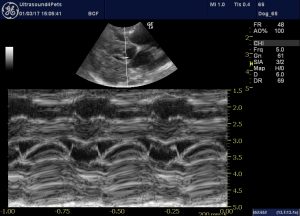
The right long axis four chamber view is markedly abnormal:
Abnormal findings include:
-RV wall hypertrophy (or pseudohypertrophy)
-RA dilation
-LV wall hypertrophy (or pseudohypertrophy)
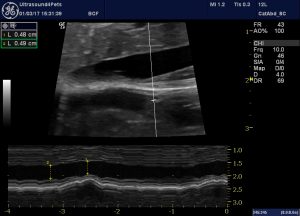
-systolic anterior motion of the septal mitral valve leaflet
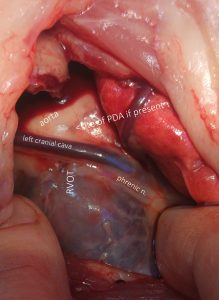
…..and, intriguingly, there is an abnormal vascular structure which is glimpsed running from the right atrium around the left atrium towards the left atrioventricular groove and then cranially.

This is the coronary sinus and it is abnormally dilated. This finding suggests that a persistent left cranial vena cava is present and is emptying into the right atrium (they sometimes go into the left).
Most often this anomaly is not associated with clinical signs. However, it’s important to know about if one is contemplating surgical closure of a patent ductus since it runs right across the left heart base between the phrenic and vagus nerves.
And multiple concurrent congenital defects are commonly encountered:
The reason for the RV hypertrophy in this cat is a double-chambered right ventricle with a muscular band circling the RV outflow tract 1cm proximal to the pulmonic valve.
There is tricuspid dysplasia with a couple of eccentric regurgitation jets:
And a small perimembranous VSD.
It is impossible to determine definitively whether left ventricular hypertrophy is a genuine hypertrophy due to outflow obstruction, pseudohypertrophy due to underfilling (secondary to reduced R heart output) or a combination of both. Similarly systolic anterior motion of the septal MV leaflet may be secondary to flattening of the ventricular septum to the left…..or indicative of an independent MV dysplasia.
R long axis view with M mode across the mitral valve leaflets showing SAM



