Pancreas of the week: no.1
To continue the problematic subject of ‘can an ultrasonographic diagnosis of pancreatitis can be made with any confidence?’, I thought I might post some images of specific cases without history and invite comments.
Maybe you’d like to score this on a scale 1 to 5 where 1 = no evidence pancreatitis and 5 = definite pancreatitis. And ideally give reasons.
There are no right or wrong answers but all interesting cases.




It’s a dog pancreas obviously: I’ll give you that much.
3
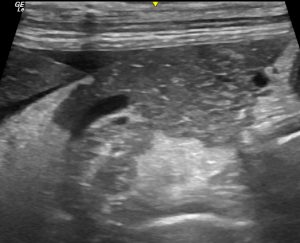
I don’t think you can form an optinion from this image. Initial inspection with local fat reaction draws the eye but looking to the left of the image the fat shows achostic enhancement and to the top right the the fat appears normal. The pancreas itself shows changes at the mid- bottom section of the image but otherwise is fairly homogenous.
I think when scanning this patient I would be looking for another cause for the fat reaction before concluding pancreatitis.
I would probably give it a 4. Although we don’t have a scale in the image, I would subjectively think the pancreas is enlarged (compared to the abdominal wall) and overall hypoechoic. The bottom margins are not regular. i agree with Ben as it looks mostly affected on the middle/bottom areas. Peripancreatic reactive fat and some free fluid around the liver border. So definitely focal peritonitis and changes in pancreas enough to be highly suspicious of pancreatitis. Of course, other causes should be ruled out before drawing conclusions.
Thanks guys, that particular dog was a CKCS with MMVD, secondary (type II) pulmonary arterial hypertension, L and R CHF. Hence the small anechoic ascitic effusion. The caudal cava was huge and not fluctuating with respiration.
I don’t have a lipase or PLI, let alone pancreatic histopath but there’s no history to suggest pancreatitis. Although he is a spaniel and undiagnosed concurrent pancreatitis is not impossible by any means.
I would be thinking that post-hepatic portal hypertension with oedema of the pancreas and abdominal fat is a plausible explanation for pancreatic hypoechogenicity and contrasting hyperechoic fat.
The ascites will also cause hyperechoic change in abdominal fat. Since that tends to be a fairly, evenly-distributed diffuse effect I suspect that it’s due to some change in the tissues. Although a purely physical effect on sound transmission also seems a possible factor to me,
If anyone knows the answer to that issue I’d be very interested. Also, thus far, I have failed to find a good explanation for why oedematous pancreas is hypoechoic but oedematous abdominal fat is hyperechoic.
The wider picture is that this kind of thing tends to make me feel that the hypoechoic pancreas/hyperechoic fat pattern isn’t specific for any one pathology.