Nasal ultrasonography -one more application for the most versatile imaging modality
There’s a certain amount of pressure as a peripatetic clinician to achieve a diagnostic outcome. The present patient is a classic of the ‘not easy’ genre. An elderly dog with recent onset inappetence-progressing-to-anorexia but lack of other specific signs. After routine anamnesis, physical examination, haematology and routine biochemistry we have:
-weight loss, inappetence
-no GI signs, no PUPD, no lameness, no cough, no fever
-increased upper respiratory noise at times, worse on stress
-mature neutrophilia 43 x 10^9/l
I won’t detail everything else which is unremarkable or within normal limits.
Normally I am thinking that in this kind of circumstance, sonography is a good next step. It’s non-invasive, doesn’t require anaesthesia, isn’t especially expensive, potentially provides a lot of of information about many body systems and is sensitive for some issues where routine bloods aren’t: such as neoplasia, infections, heart failure.
This patient’s lungs look good -reinforcing the impression that any respiratory issues might be upper respiratory. Pneumonias are always a strong contender for neutrophilia in aged dogs and don’t always cause obvious, specific external signs. Sonography is useful here since the evidence suggests that it has quite a high negative predictive value for pneumonia.
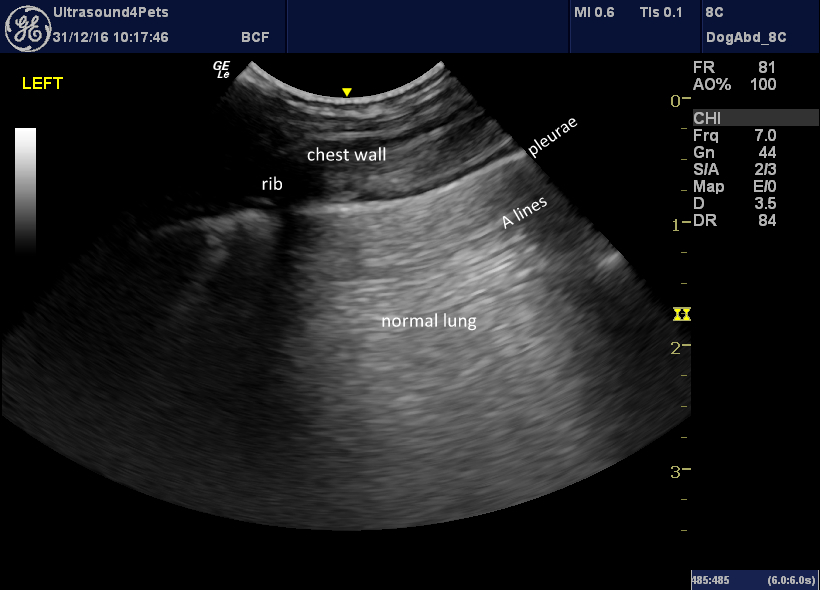
longitudinal plane transthoracic view of lung
Likewise, cardiac chambers are broadly in normal proportions: it is unlikely that heart failure is the primary cause of malaise:
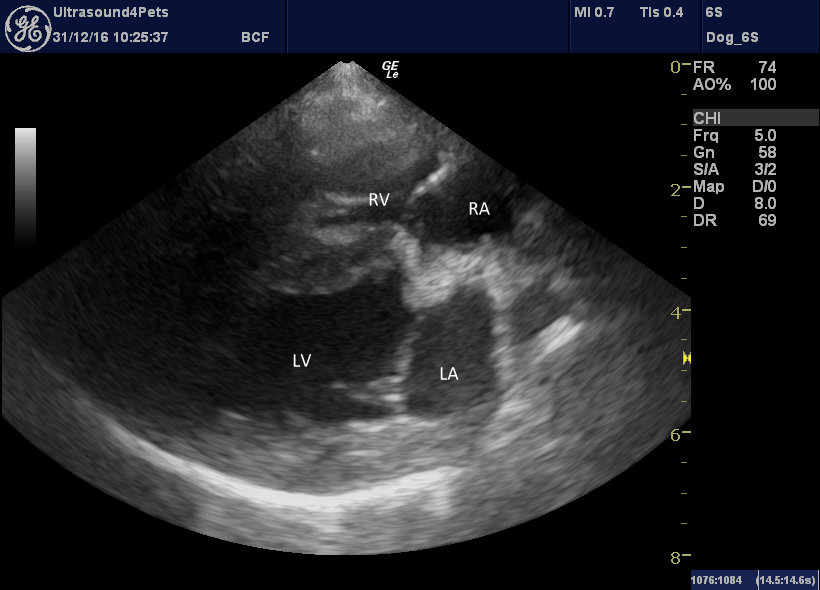
right, long-axis, four-chamber view of heart
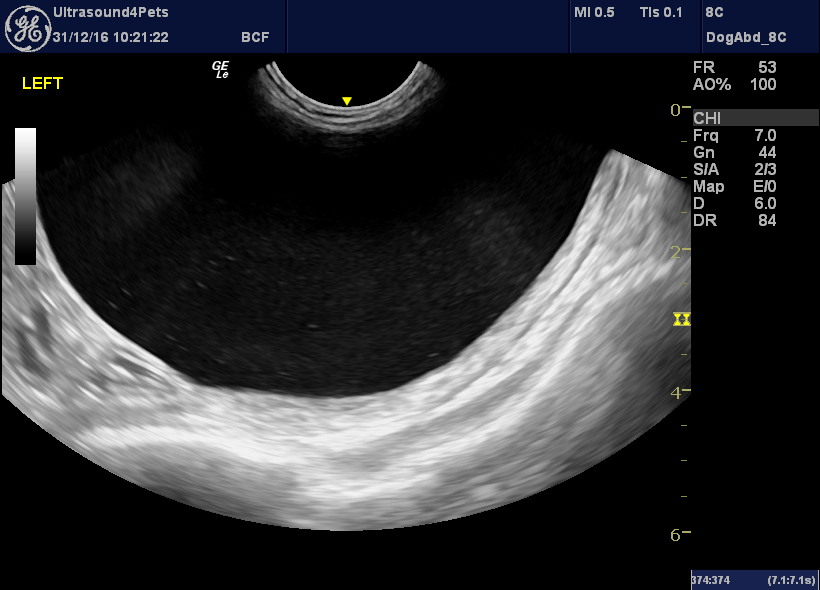
In the abdomen, the gallbladder is interesting:

There is a thick, immobile, hypoechoic peripheral zone which is likely to be mucus and central hyperechoic bile. This is probably an incomplete mucocoele. This could conceivably be associated with inappetence, abdominal, pain or vomiting. However, this dog’s liver enzymes are not elevated. There is no evidence of inflammation around the gallbladder to suggests cholecystitis or incipient rupture and, this being the case, I think it’s a bit unlikely that biliary pathology is responsible for a severe neutrophilia and complete anorexia.
In the bladder, there’s a little sediment…
Who knows…..could be a UTI…..even pyelonephritis. The kidneys have the kind of loss of cortico-medullary distinction which is common in older dogs.
Pyelonephritis is a bit of a problem area as far as I’m concerned: there isn’t much published and some authoritative sources have stated that any UTI in a dog should be treated as potential pyelonephritis. See IRIS guidelines for example. Does that mean they should all get 6-8 weeks oral antibiotics????
Urine sediment microscopy is rather underwhelming in this case though: just a few cellular casts. There were no bacteria but antibiotics have already been given.
In the event of diagnostic stagnation it’s always go advice to go back to the patient. This dog has fairly convincing upper respiratory issues at times: it’s just that it initially seemed unlikely that they were responsible for the full extent of the current problem.
So, on more detailed examination there is a small ‘puffy’ area at the caudal end of the bridge of the nose.

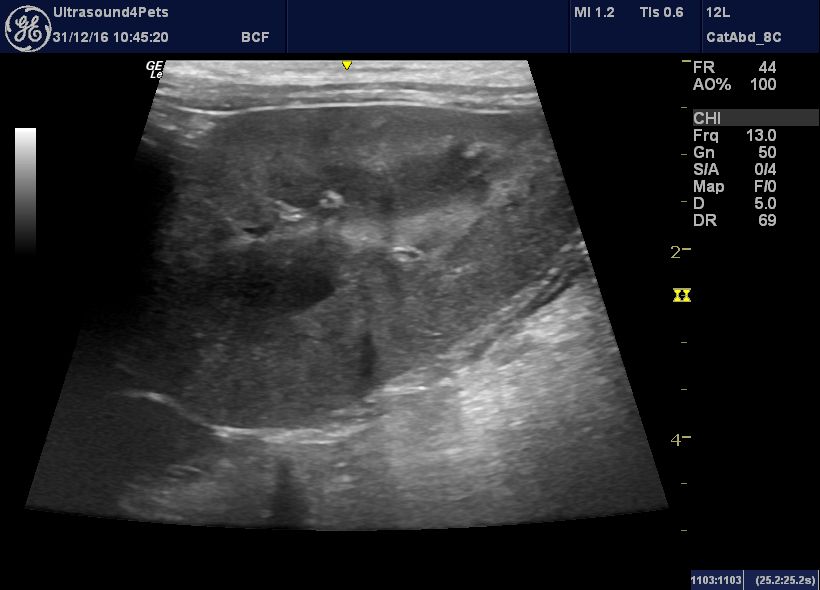
Applying a linear probe here:
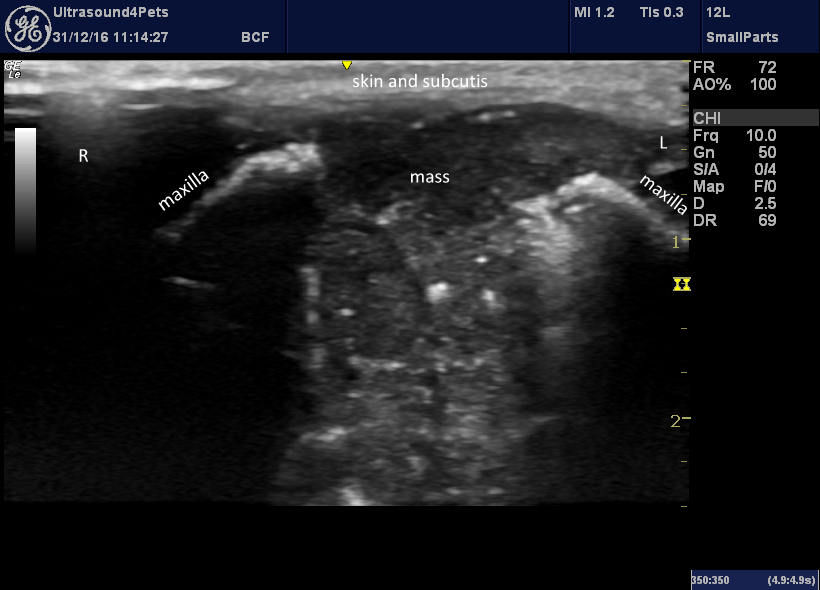
transverse view of base of bridge of nose
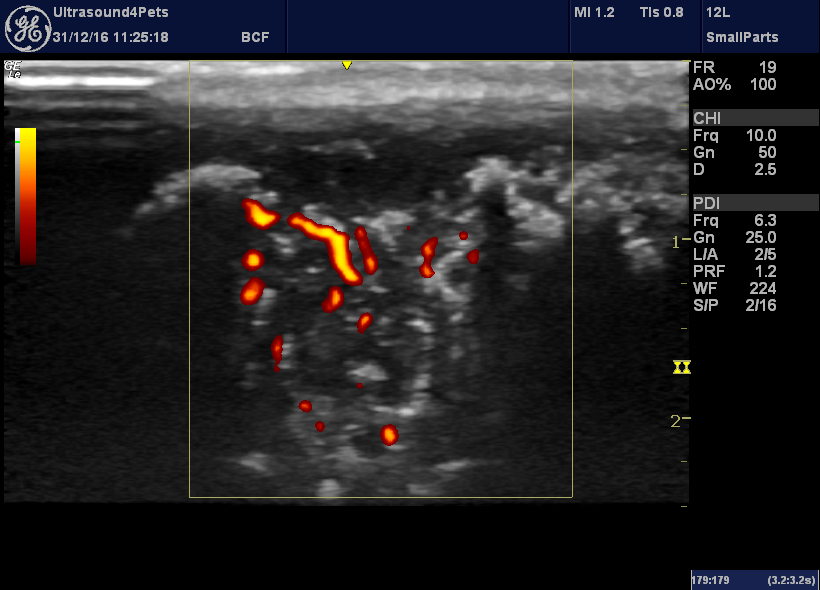
The same view with power Doppler to confirm vascularity
That looks awful! On either side is the reflective surface of the remaining parts of the maxillae. Centrally there is a 10mm gap with complete erosion of bone. This space is occupied by fairly homogeneous soft tissue which fills the visible part of the nasal cavity and spills out dorsally into the subcutaneous tissue.
On a longitudinal view:
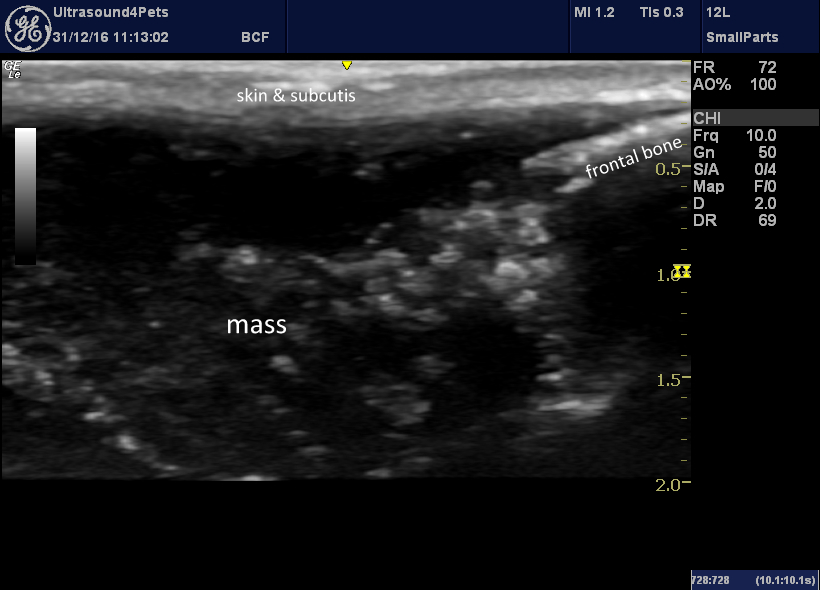
longitudinal view of same area with rostral to left of image
The rostral end of the frontal bone ends abruptly.
On radiography, bony changes are confirmed:

This seems overwhelmingly likely to be the cause of this poor dog’s problem. We didn’t get to investigate further but I presume that a nasal neoplasm was responsible (with fungal rhinitis perhaps a distant second possibility).



