Gallbladder mucocoele complications
Gallbladder mucocoeles are often a decision-making dilemma. Frequently they are incidental findings. Very occasionally they are secondary to hypothyroidism -in which case resolution with medical treatment is reported:
http://www.ncbi.nlm.nih.gov/pubmed/18518811
Otherwise, it’s a matter of surgery or wait and hope for the best. Personally I usually advise surgery if there are compatible clinical signs. If the patient is asymptomatic then waiting often seems reasonable…..unless things get complicated.
Principally these come in 3 varieties:
- rupture
- septic cholecystitis
- rupture with sepsis
Although, cholecystectomy is likely to be the long term answer in both scenarios my experience is that purely septic scenarios are best managed acutely with aggressive antibiotics until surgery can be performed in a stable patient at a later date. Whereas ruptures (with or without sepsis) are best treated surgically as soon as circulatory and metabolic derangements are adequately controlled (usually within a few hours) to minimise further bile peritonitis.
Ultrasonographically, cranial abdominal fat is likely to be hyperechoic in both circumstances:
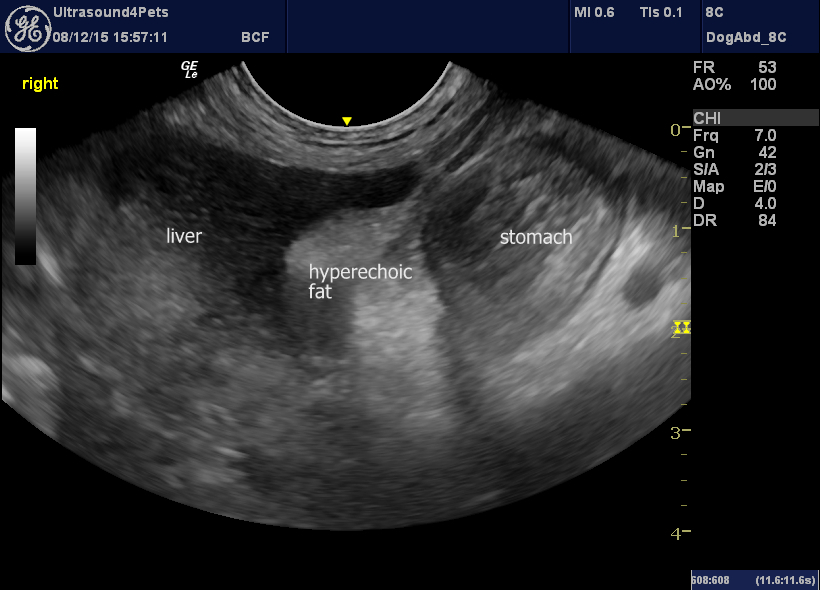
sagittal plane view of the cranial abdomen with liver, stomach body and porta hepatis area in between. Abdominal fat is markedly hyperechoic to the liver.
Cholecystitis cases often have no (or small) effusion in my experience. Rupture tends to cause a localised effusion extending along the lesser curvature of the stomach.
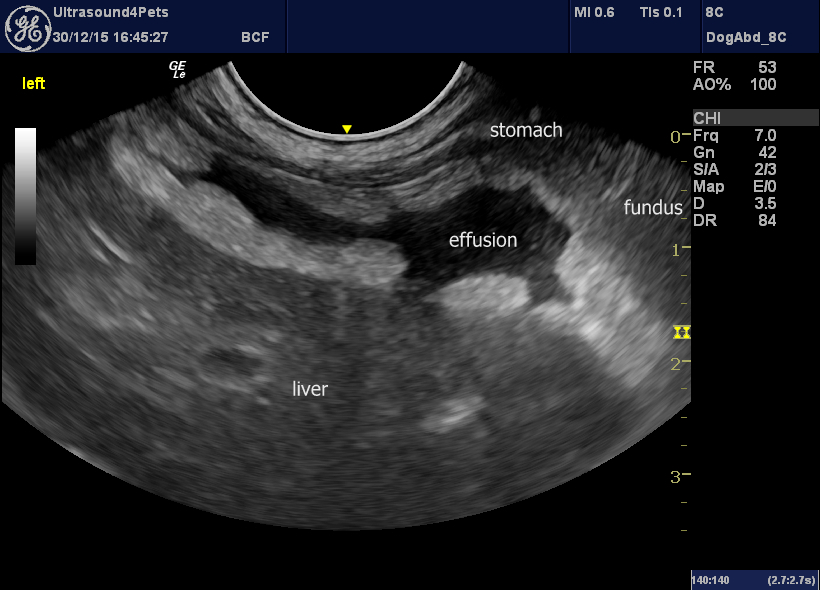
transverse plane view of the cranial abdomen from the ventral midline caudal to the xiphisternum. There is a localised effusion between liver and lesser curvature of stomach with intensely hyperechoic abdominal fat surrounding.
This localisation is less common in pancreatitis.
Aspirates of effusion are useful to assess for the presence of bile, bacteria or both. Comparing blood and effusion glucose levels is useful to further assess likelihood of sepsis when no bacteria are visible.
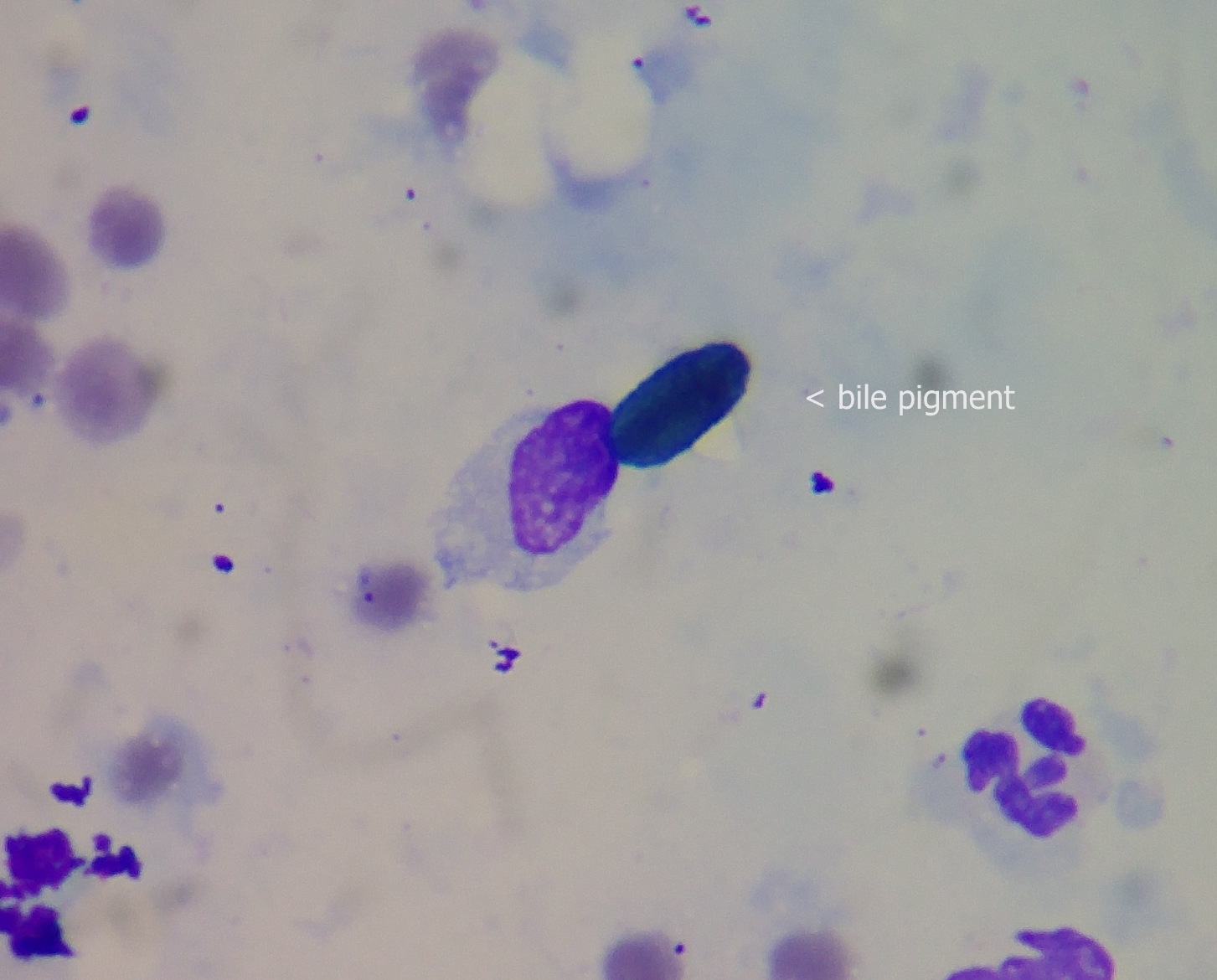
Rapi-Diff stained cytology of abdominal effusion from a dog with gallbladder rupture. Pigmented biliary granules are present. Absence of pigmented bile does not prove absence of rupture.
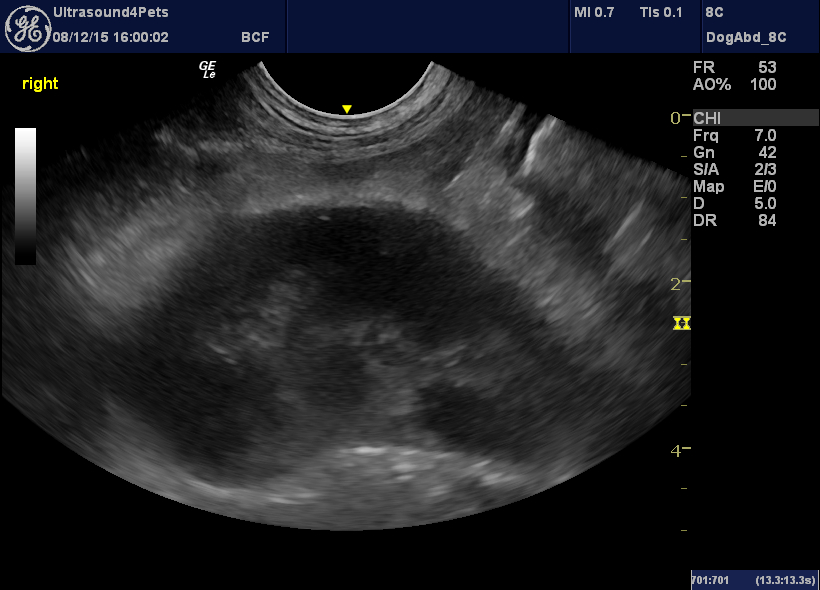
Gas densities or intense hyperechoic change around the gallbladder indicate sepsis:
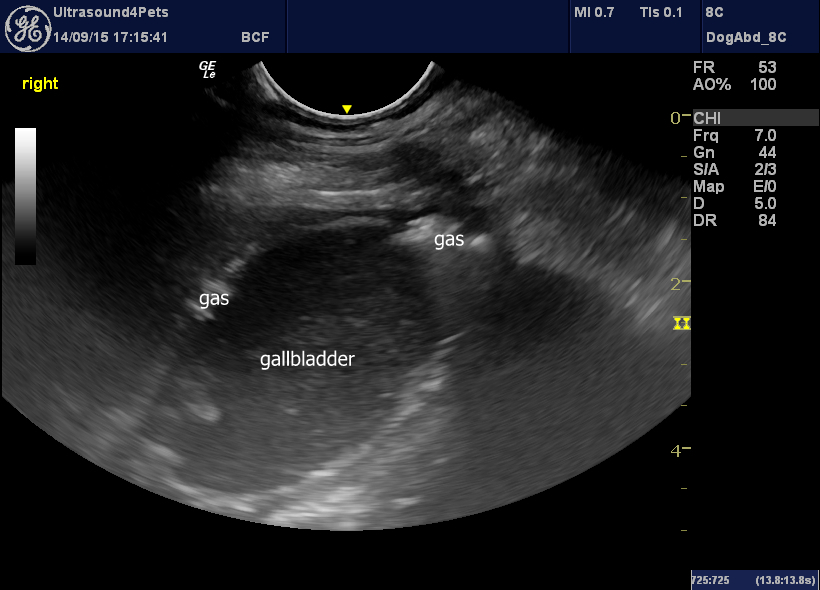
oblique view of the gallbladder in a dog with septic non-ruptured gallbladder mucocoele
another similarly-affected dog without gas densities
All of the dogs whose images appear here were Border Terriers. In our part of the UK a Border Terrier with an acute abdomen warrants ultrasonography at an early opportunity.



