Focus on testicles
One of the cardinal rules of serious small animal sonography is ‘don’t forget to scan the ovaries, uterus and testicles’. At least in the UK it’s easy to forget that they’ve not always been removed!.
A couple of recent examples:
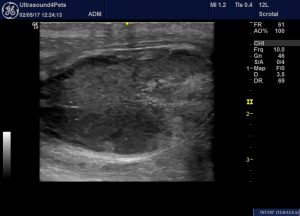
Firstly a young unilaterally-cryptorchid dog presented with acute abdominal pain. Impressively, the first opinion practitioner suspected a testicular torsion from first presentation.

oblique view of the abdominal testicle in the caudal abdomen. There is a local effusion, the epididymis is swollen and power Doppler reveals reduced perfusion.
This appearance is very similar to the ultrasonographic appearance reported in man:
http://emedicine.medscape.com/article/381204-overview

The offending gonad at surgery
Secondly: a middle-aged entire male Labrador presenting with antibiotic-responsive fever of 40.5C. However, relapse followed a few days after cessation of a five-day antibiotic course. Abdominal findings were largely unremarkable except that the right renal pelvis was mildly dilated:

transverse plane view of the right kidney. The pelvis shouldn’t normally exceed 2mm.
Renal cortical echogenicity might be judged somewhat hyperechoic and heterogeneous compared to normal.
The prostate is ‘large’ (as would be expected in an entire male of this age) with diffusely heterogeneous parenchyma, small cystic areas but no marked asymmetry or discrete lesions of any appreciable size.

transverse view of the prostate
However, the testes are markedly asymmetrical and abnormal:

long axis view of the cranial pole of the right testis showing a discrete hyperechoic lesion

caudal pole and (normal-looking) epididymis of the right testis
The left testis: there is are irregular, multi-focal, heterogeneous but predominantly hyperechoic abormal areas

left testis: caudal pole and epididymis. The testis is abnormal in this view also. The epididymis is swollen and very heterogeneous with irregular hypoechoic areas
These findings were considered most consistent with right testicular neoplasia, left testicular orchitis and epididymitis. In view of the probability of neopalsia, the severity of systemic signs and incomplete response to broad spectrum antibiotics bilateral castration was performed.
Bacterial culture from the abnormal epididymis yielded a profuse growth of an E. coli sensitive to most standard antibiotics.
Histopathology confirmed bacterial orchitis, epididymitis on the left and seminoma plus interstitial cell tumours in the right testis.
It seems likely that in this case the source of infection may have been bacterial UTI with possible pyelonephritis (which would account for renal pelvic dilation) and/or prostatitis.



